I stumbled across this short video clip the other day. It shows Scott Morrison talking to Jo Howes about how we should try to turn problems into puzzles.
I really liked how there might be an alchemy associated with just changing the word we use to describe it. No need to get into the actual definition of a 'problem' versus the actual definition of a 'puzzle'. Just use the word 'puzzle'.
And I thought: we need to re-frame 'The Patient Flow Problem' as 'The Patient Flow Puzzle'.
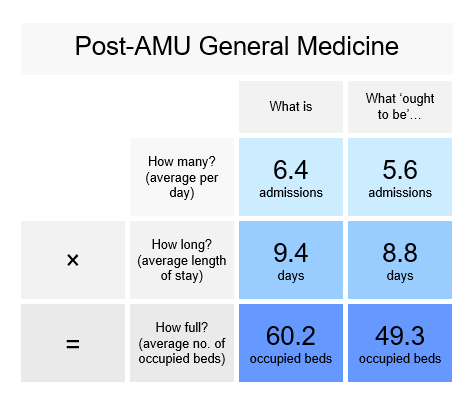
Or maybe: each hospital specialty should have its own puzzle. For example, this is the specialty of post-AMU General Medicine. Its 'puzzle' is that it needs to find a way of changing its numbers from the numbers in the column on the left to the numbers in the column on the right.
That's it! It's just a puzzle! (And yes, I know there's a lot more to it than that! And yes, I know, I'm just a data analyst, all I have to do is tell you what the numbers are; I don't have to tell you what to do to change them. But at least just having the numbers would be a start!
I'm even tempted to make those blue squares into actual game tiles (like in Scrabble or whatever) to emphasize the 'puzzle-ness' of it! The important thing is to re-frame the problem as a puzzle. Psychologically, people don't like problems. But they do like puzzles.
Like Scott Morrison says in the video, we gravitate towards puzzles. We're happy to help someone with their Sudoku, their crossword, their jigsaw... ...but we run a mile from their problems!
Furthermore, if we show clinicians the 'puzzle principles' (i.e. how length of stay and admission rates can interact in different ways to generate different levels of bed occupancy), we can help them figure out the puzzle for themselves, or at least give them the tools to start figuring it out.
There's something else about puzzles. Yes, they have this appearance of being straightforward, but they demand accuracy. You can't solve puzzles approximately. You can't describe the first two 'what is' numbers in this example with the words "approximately six admissions a day, length of stay approximately nine days". Because if you did, you'd find that you were also describing the 'what ought to be' numbers.
You'd be describing both misery and happiness with the same numbers! Even Mr Micawber knew it was important not to round, that it was just a shilling that made all the difference!
So with average length of stay for example, it'd be really important to know if you're aiming for 8.8 days as opposed to sticking with 9.4 days. You can't just say "nine" and hope for the best! Puzzles demand accuracy. You've got to spell words accurately in a crossword. There's no room for approximation in Sudoku!
So what we're saying to each clinical director is: "You only need to know six numbers. Three 'what is' numbers. And three 'what ought to be' numbers.
But you really need to know them! To two decimal places!
Flow_ology can be booked as an on-site face-to-face course for £1,250+VAT, and up to 12 participants can be accommodated in each workshop session. Email info@kurtosis.co.uk to start making arrangements. Open course places cost £350+VAT.